
Supraspinatus Tendon Tears: Imaging Diagnosis, Ultrasound and Clinical Management
- Dr. Segnini

- Mar 16
- 3 min read
Supraspinatus tendon tears represent the most prevalent pathology of the rotator cuff, accounting for 51% to 77% of all tendinous shoulder ruptures. Accurate imaging diagnosis is critical for therapeutic decision-making and the patient's functional prognosis.
Functional Anatomy of the Supraspinatus Tendon
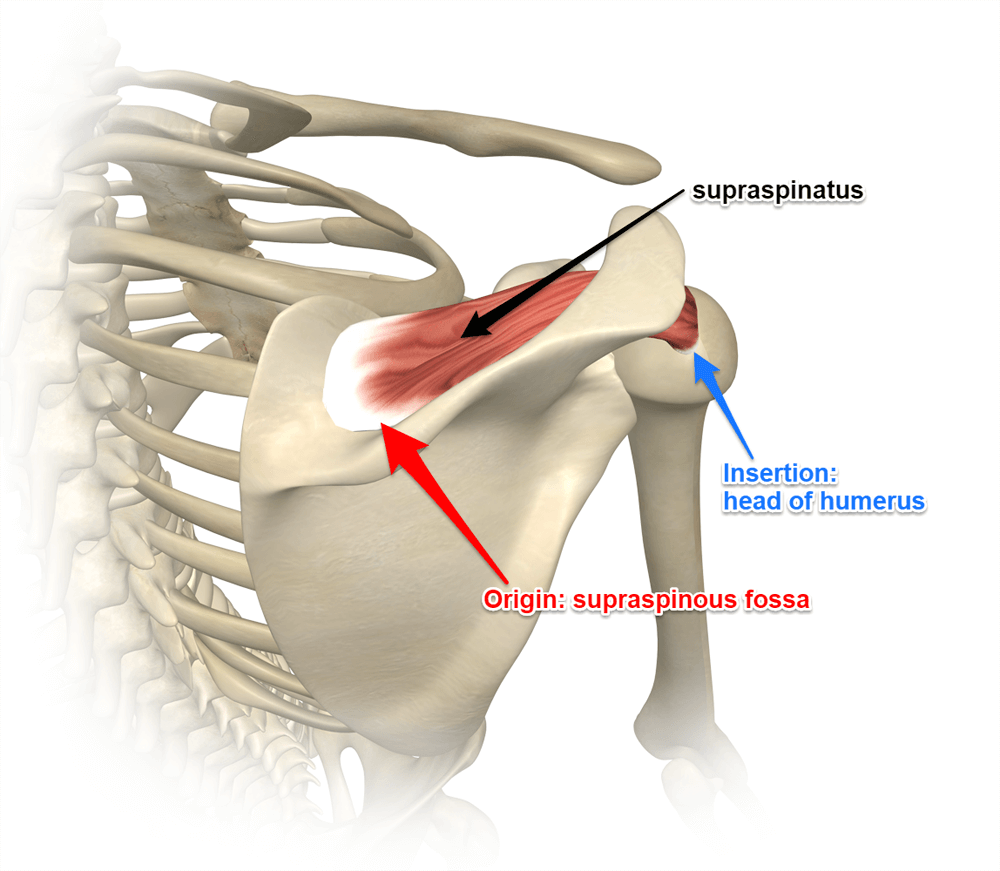
The supraspinatus muscle originates from the supraspinous fossa of the scapula, and its tendon courses through the subacromial space, inserting onto the superior facet of the greater tuberosity of the humerus. Codman's critical avascular zone is located 1 cm proximal to the distal insertion, where repetitive mechanical tension and relative hypovascularity predispose to fibrillar degeneration and eventual rupture.
Biomechanically, the supraspinatus acts as the initiator of glenohumeral abduction (0–15°), working synergistically with the deltoid. As a component of the concentric compression mechanism, it stabilizes the humeral head against the glenoid during movement. Its dysfunction alters scapulohumeral rhythm and predisposes to secondary injuries of the infraspinatus tendon, long head of biceps brachii, and glenoidal labrum.
Classification of Supraspinatus Tears
The most widely used classification distinguishes between partial-thickness and full-thickness tears. Partial tears are subclassified by location: bursal surface (PASTA type: Partial Articular Supraspinatus Tendon Avulsion), articular surface, or intratendinous. The Ellman classification grades partial tears in three degrees based on the depth of tendon involvement:
Grade I (Ellman I): depth ≤3 mm — superficial lesion without significant functional impairment
Grade II (Ellman II): depth 3–6 mm — involvement of up to 50% of the tendon thickness
Grade III (Ellman III): depth >6 mm — involvement exceeding 50% of tendon thickness, frequently requiring surgical intervention
Full-thickness tears are classified by anteroposterior diameter: small (<1 cm), medium (1–3 cm), large (3–5 cm), and massive (>5 cm or involvement of two or more tendons). This grading has direct implications for surgical indication and arthroscopic reparability potential.
Sonographic Findings: High-Resolution Ultrasound
High-resolution musculoskeletal ultrasound with a 12–18 MHz linear transducer is the first-line modality for supraspinatus tendon evaluation, with sensitivity and specificity comparable to MRI for full-thickness tears (sensitivity: 89–100%; specificity: 85–98%). Its advantage lies in real-time dynamic exploration and immediate contralateral comparison.

In articular surface partial tears, a focal hypoechoic or anechoic defect is identified on the deep tendon surface without communication with the subacromial-subdeltoid bursa. The bare cartilage sign and loss of articular contour convexity are additional diagnostic criteria. A full-thickness tear is characterized by transmural discontinuity with glenohumeral-bursal communication, the bare articular cartilage sign — virtually pathognomonic — and the delta sign (bursal depression).
MRI: Correlation with Sonographic Findings
Shoulder MRI, preferably with arthrography (MR arthrography) for partial lesions, provides superior information regarding anteroposterior tear extension, degree of tendon retraction, muscle atrophy, and fatty infiltration (Goutallier classification). ABER sequences increase sensitivity for PASTA lesions to 89%. Proximal humeral head migration with subacromial space reduction (<6 mm) suggests massive tear with Hamada stage III–V cuff arthropathy.
Clinical-Imaging Correlation and Therapeutic Management
Subacromial impingement syndrome (positive Neer and Hawkins-Kennedy tests), painful arc limitation between 60–120°, and weakness on Jobe's empty can test are the semiological findings correlating with supraspinatus pathology. Clinical-sonographic correlation is essential, given that asymptomatic tears in patients over 60 years reach a prevalence of 30–50%.
Conservative treatment (physical therapy, NSAIDs, ultrasound-guided corticosteroid or PRP injection) is indicated for Ellman I–II partial tears and small full-thickness tears in low-demand patients. Arthroscopic repair is the standard for medium and large tears in active patients, with better outcomes achieved before Goutallier stage III–IV muscle atrophy.
Orthopedic Support Devices for Shoulder Injuries
Need an Online Radiological Second Opinion?
Imaging diagnosis of supraspinatus tendon tears requires precise knowledge of sectional anatomy, sonographic and MRI criteria, and correlation with the patient's clinical context. High-resolution dynamic ultrasonography and MR arthrography remain the imaging pillars of rotator cuff assessment in advanced musculoskeletal practice.



Comments