
Achilles Tendinopathy: Complete Clinical Guide for Healthcare Professionals and Patients
- Dr. Segnini

- Mar 16
- 3 min read
Achilles tendinopathy is one of the most frequent conditions in sports medicine and orthopedics, with an annual incidence of 2.35 per 1,000 in the general population and up to 10 times higher in elite runners. Understanding its pathophysiology, imaging classification, and therapeutic options is essential for both healthcare professionals who diagnose it and the patients who suffer from it.
Anatomy and Biomechanics of the Achilles Tendon
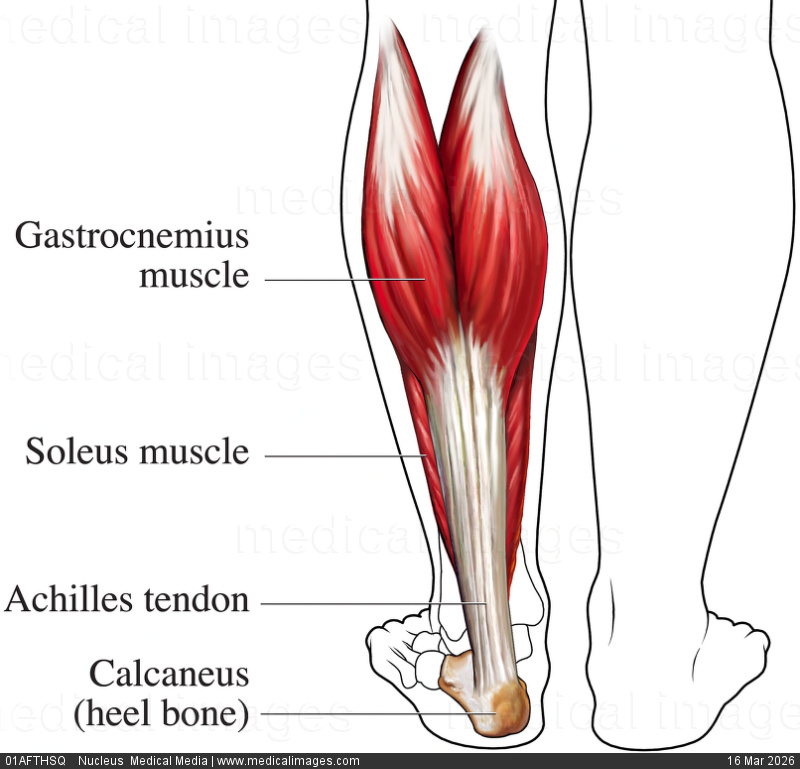
The Achilles tendon is the most robust tendon in the body, formed by the confluence of the medial gastrocnemius, lateral gastrocnemius, and soleus tendons (triceps surae musculotendinous complex). It inserts onto the posterosuperior aspect of the calcaneus after a 90° counterclockwise rotation on its longitudinal axis. This intrinsic torsion generates a hypovascular zone between 2 and 6 cm proximal to the calcaneal insertion — the critical zone — where the majority of degenerative ruptures occur.
Biomechanically, the Achilles tendon transmits forces of up to 12.5 times body weight during running. Tendinopathy arises when repetitive mechanical load exceeds the tissue's repair capacity, triggering fibrillar degeneration, pathological neovascularization, and adipose infiltration — hence the term tendinosis.
Clinical and Imaging Classification
Three main presentations are distinguished: non-insertional tendinopathy (critical zone, 2–6 cm proximal to insertion), insertional tendinopathy (calcaneal enthesis, associated with retrocalcaneal bursitis and Haglund deformity), and paratendinitis. The Nirschl-Alfredson classification grades severity in four stages. The Kuwada classification grades tears: Type I (partial <50%), Type II (partial >50%), Type III (complete, diastasis <3 cm), and Type IV (complete, diastasis >3 cm).
Sonographic Diagnosis: High-Resolution Ultrasound
High-resolution musculoskeletal ultrasound with a 12–18 MHz linear transducer is the first-choice diagnostic modality. The normal tendon displays a hyperechoic parallel fibrillar pattern with a maximum anteroposterior diameter of 6 mm. In tendinosis: fusiform thickening (>6 mm), loss of fibrillar pattern, intrasubstance hypoechoic foci, intratendinous calcifications, and pathological neovascularization on color Doppler. A complete tear shows total discontinuity with hemarthrotic gap filling and proximal stump retraction.
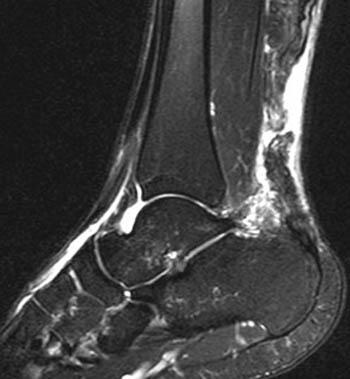
MRI: Staging and Surgical Planning

MRI is indicated in suspected complete rupture, preoperative planning, and complex insertional tendinopathy evaluation. Preferred sequences are sagittal T1, T2, and STIR. A complete tear shows tendon discontinuity with hyperintense signal in the T2/STIR gap, proximal stump retraction, and peritendinous edema. MRI provides critical surgical planning data: gap length, residual degeneration, paratenon integrity, and Haglund deformity morphology.
What Patients Need to Know: Warning Signs and When to Seek Care
If you experience pain at the back of the heel or ankle — especially on first morning steps, climbing stairs, or after exercise — you may have early Achilles tendinopathy. Seek urgent specialist evaluation if you feel sudden intense heel pain after a jump or run, cannot bear weight, or feel a palpable depression along the tendon. These signs may indicate a complete rupture requiring immediate imaging evaluation.
Therapeutic Options: From Conservative Treatment to Surgery
The Alfredson eccentric protocol (3 sets of 15 repetitions twice daily for 12 weeks) has the strongest evidence in chronic non-insertional tendinopathy, with 80–90% success rates. Ultrasound-guided PRP injection is indicated for refractory tendinosis at 12 weeks. Doppler-guided Polidocanol injection (Ohberg technique) targets pathological neovascularization. Surgical repair is indicated for Kuwada III–IV tears and refractory insertional tendinopathy.
Orthopedic Support Devices for Achilles Tendon Conditions
Do You Have Images and Need a Radiological Second Opinion?
Achilles tendinopathy demands a multimodal diagnostic approach integrating clinical assessment, high-resolution dynamic Doppler ultrasound, and MRI when indicated. Precise anatomoclinical and imaging correlation allows selection of the optimal therapeutic strategy — from eccentric protocol to reconstructive surgery — ensuring the best functional prognosis for each patient.


Comments