
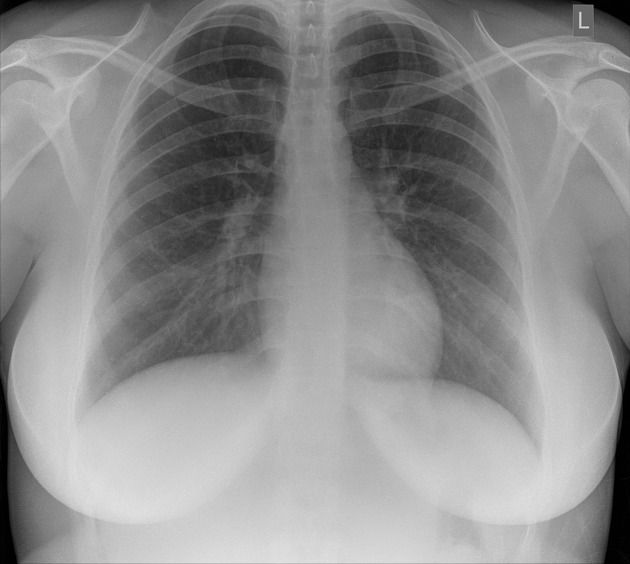
PA and Lateral Chest X-ray: Optimal Technique, Quality Criteria, and Systematic Interpretation. PA chest x-ray
- Dr. Segnini

- Mar 19
- 6 min read
Clinical Introduction
The posteroanterior (PA) chest radiograph with lateral views is the most frequently requested imaging study worldwide, representing approximately 30–40% of all conventional radiological examinations. Its diagnostic role ranges from screening for pleuropulmonary pathology to monitoring chronic cardiovascular diseases, postoperative management of implantable devices, and the initial assessment of critically ill patients.
Despite its apparent technical simplicity, chest radiography is one of the studies with the highest rate of diagnostic error due to acquisition deficiencies: patient rotation, submaximal inspiration, inadequate kilovoltage, and incorrect collimation are the factors that most frequently compromise diagnostic quality. This article answers a fundamental clinical question: what technical and interpretative conditions are necessary for a chest radiograph to be diagnostically valid?
Relevant Radiological Anatomy
Lung parenchyma: The lung fields are divided into thirds (upper, middle, and lower) and zones (inner, middle, and peripheral). The bronchovascular markings should be visible up to the outer two-thirds of the parenchyma; their peripheral absence suggests hyperinflation or pneumothorax, while their accentuation may reflect vascular congestion or fibrosis.
Cardiovascular silhouette: In PA projection, the normal cardiothoracic ratio (CTR) is ≤0.50 in adults with adequate inspiration. The prominence of the aortic arch, pulmonic knob, and cardiac borders should be assessed as individual units.
Mediastinum: Its maximum width at the aortic level should not exceed 8 cm. The trachea is identified as a central air column with a slight deviation to the right at the level of the aortic arch (normal variant).
Normal variants not to be confused with pathology: accessory azygos fissure, pectus excavatum simulating cardiomegaly in AP projection, prominent breast simulating pulmonary opacity, costal osteophytes simulating nodules, costochondral calcifications vs. solitary pulmonary nodule.
Radiological Technique and Acquisition Protocol
Patient positioning — Standard PA projection
The patient stands upright, with their chest in contact with the detector (wall bucky), arms internally rotated, hands resting on their hips, and elbows forward—a maneuver that displaces the scapulae laterally, away from the lung fields. The chin should be raised slightly to prevent the soft tissue shadow of the neck from projecting onto the apices.
The sagittal plane must be strictly perpendicular to the detector plane, with both shoulders at equal distances from the edge of the receiver. Rotation is the most frequent positional artifact and the one that most compromises the evaluation of the cardiovascular silhouette and the pulmonary hila.
Left lateral projection
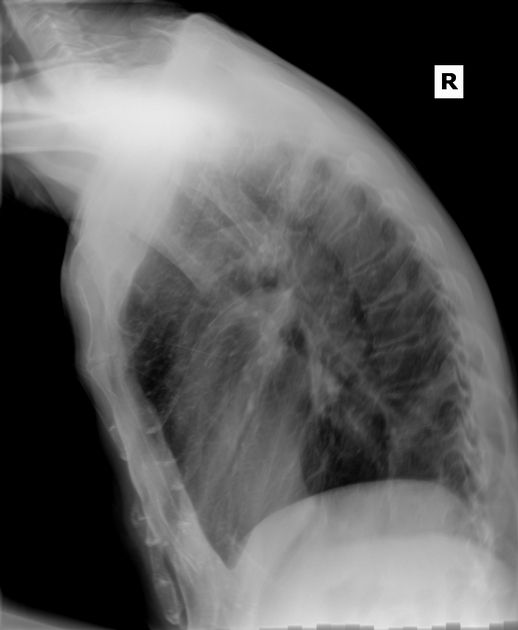
The left hemithorax rests on the detector to minimize cardiac magnification. The arms are raised above the head and held on a support bar. The feet are slightly separated to ensure stability. The right lateral projection is reserved for characterizing lesions of the right middle lobe or when left-sided pathology requires greater detail.
Central ray and angulation
PA: Horizontal central ray, perpendicular to the detector, centered at the T6–T7 level (inferior angle of the scapula in standard position). No cephalic or caudal angulation. The lordotic projection (AP with 15° cephalic angulation) is complementary for vertices and middle lobe — not a substitute for the conventional PA.
Recommended Technical Parameters
PA Projection — kVp: 110–125 | mAs: 4–6 (AEC) | DFR: 180 cm (min. 150 cm) | Grid ≥10:1 | Time <20 ms
Lateral Projection — kVp: 110–125 | mAs: 16–20 (AEC) | DFR: 180 cm | Grid ≥10:1 | Time <40 ms
Critical technical note: The use of high kVp (≥110 kVp) is mandatory in the thorax. This allows adequate penetration of the mediastinum and thoracic spine without overexposing the lung parenchyma. With kVp <90 kVp, the thoracic spine remains unpenetrated and retrocardiac structures are undetectable.
Image Quality Criteria
A PA chest X-ray must meet ALL of the following criteria before being accepted for reporting:
Inspiration: Right hemidiaphragm at the level of the 6th anterior rib or 10th–11th posterior rib. Submaximal inspiration produces apparent cardiomegaly and accentuation of the basal pattern.
Rotation: Clavicle heads equidistant from T3–T4 spinous processes. Asymmetric distance >1.5 cm invalidates evaluation of mediastinum and hila.
Penetration: Dorsal vertebral bodies barely visible through the cardiac shadow (T4–T8); vascular pattern visible in retrodiaphragmatic lung bases.
Collimation: Field that includes lung apices, costophrenic sinuses and lateral chest wall, without sectioning diagnostic structures.
Clarity: No blurring due to respiratory motion. Cardiovascular borders and diaphragm are sharp. PA chest radiograph
OPERATIONAL CHECKLIST — PA AND LATERAL CHEST X-RAY
Medical request verified and patient data confirmed
Clothing and metal objects removed (necklaces, underwire underwear, transdermal patches)
Patient in firm standing position — check stability
Thorax in contact with the detector — DFR = 180 cm verified
Hands on hips, elbows projected forward (scapular displacement)
Shoulders at equal distance from the edge of the detector (rotation control)
Chin elevated — lung apices free of soft tissue shadowing
Clear verbal instruction: 'Take a deep breath… hold your breath… don't breathe'
Exposure in maximum inspiratory apnea
Immediate verification: inspiration, rotation, penetration, collimation — criteria met → accepted | not met → repeat with documented correction
Systematic Radiological Interpretation — ABCDE Method. PA chest radiograph

Unsystematic reading is the most frequent cause of diagnostic error by omission. The use of a structured method is recommended regardless of the informant's level of experience.
A — Airway: Trachea in midline, carina at T4–T5 level, subcarinic angle <70°, main bronchi patent.
B — Bones and soft tissues: Systematic review of ribs 1st–12th, clavicles, scapulae, proximal humeri, thoracic spine. Subcutaneous emphysema: banded radiolucency in soft tissues.
C — Cardiac silhouette: ICT ≤0.50, cardiac shape and borders, aortic knob, aortopulmonary window, main pulmonary arch.
D — Diaphragm and costophrenic angles: Right hemidiaphragm 1.5–2.5 cm higher than the left. Acute costophrenic angles. Blunting indicates >200–300 mL of pleural fluid.
E — Everything else: Lung parenchyma by zones and fields. Hila (position, size, density). Pleural spaces. Superior mediastinum. Implantable devices.
Classic Radiological Signs
Silhouette sign: Loss of the cardiovascular border adjacent to an opacity. Right cardiac border → middle lobe; left cardiac border → lingula; right hemidiaphragm → right lower lobe.

Air bronchogram sign: A tubular air-filled image within an opacity—indicates alveolar consolidation (patent bronchus, occupied alveolus). Present in pneumonia, alveolar edema, and bronchioloalveolar carcinoma.

Meniscus sign: Homogeneous opacity with a concave upper border in the costophrenic angle — characteristic of free pleural effusion on PA projection.

Kerley B lines: Horizontal linear opacities <2 cm in the lung bases, perpendicular to the pleura. Indicative of septal interstitial edema—heart failure with PCWP >18–20 mmHg.

Common Pitfalls in Interpretation
Normal thymus in infant vs. anterior mediastinal mass: Sail sign; wavy borders; disappears in >2 years.
Breast overlap at the base vs. consolidation: Bilaterally symmetrical, diffuse lower border. Review lateral projection.
Pectus excavatum vs. cardiomegaly: Lateral sternal depression; heart displaced to the left.
Submaximal inspiration vs. actual cardiomegaly: Repeat at deep inspiration; ICT normalizes.
Rib calcification vs. pulmonary nodule: Oblique projection or CT for definitive differentiation.
Multimodal Correlation and Second Radiological Opinion
Chest X-ray has a sensitivity of 43–74% for consolidations <1 cm. Point-of-care pleural ultrasound (POCUS) has superior sensitivity for effusions ≥20 mL and can identify loculation and guide thoracentesis. Any diffuse interstitial lesion without a clear etiology, pulmonary nodule ≥6 mm, suspected pulmonary embolism, or atypical effusion requires contrast-enhanced CT.
Do you have doubts about the interpretation of a complex chest X-ray? At www.drsegnini.com you can request a second radiological opinion online with a specialized report in 24–48 hours.
Key Points — Take-Home Messages
Mandatory DFR of 180 cm in PA projection. Portable AP projection magnifies the mediastinum up to 20% — explicitly document this in the report.
Optimal kVp: 110–125 in adults. Below 100 kVp the mediastinum and thoracic spine remain unpenetrated.
Right hemidiaphragm at the level of the 6th anterior rib = minimum acceptable marker of inspiration. Repeat if inspiration is deficient unless contraindicated.
The silhouette sign is the most powerful anatomical localization tool in conventional chest radiology. It should be applied systematically before issuing a topographic diagnosis.
All portable AP X-rays in the ICU must be reported with an explicit warning: AP projection, reduced DFR, supine position.
Lung ultrasound and chest X-ray are complementary in critically ill patients. Neither replaces the other.
Incidentally detected pulmonary nodule ≥6 mm requires follow-up protocol with low-dose CT (Fleischner Society guidelines 2017).
Bibliographic References (Vancouver)
Franquet T, Giménez A, Rosón N. Chest Radiology: A Practical Guide. 3rd ed. Madrid: Médica Panamericana; 2021.
Hansell DM, Lynch DA, McAdams HP, Bankier AA. Imaging of Diseases of the Chest. 5th ed. Philadelphia: Elsevier Mosby; 2022.
American College of Radiology (ACR). ACR–SPR Practice Parameter for the Performance of Thoracic Radiography. Revised 2022. Reston, VA: ACR; 2022.
Herring W. Learning Radiology: Recognizing the Basics. 4th ed. Philadelphia: Elsevier; 2020.
MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology. 2017;284(1):228–243.
European Society of Radiology (ESR); EFRS. Patient safety in medical imaging. Insights Imaging. 2019;10(1):45.
Reed JC. Chest Radiology: Plain Film Patterns and Differential Diagnoses. 6th ed. Philadelphia: Elsevier; 2018.
Comments